
Osteopath Robert Shanks is the co-founding Clinical Director of Spine Plus, group of multi-disciplinary clinics in London (Harley Street) and Essex.

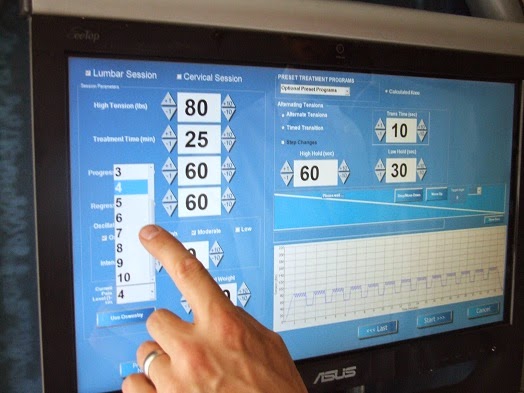
Around 2008 I began hearing about Intervertebral Differential Dynamics (IDD) Therapy, a non-surgical spinal decompression treatment which appeared to address the failings of traction quite systematically. These sophisticated IDD treatment machines were developed in the US in the late Nineties by a team of engineers and clinicians whose aim was to mechanically decompress the disc by improving upon traditional traction methods.


A typical patient is 63 year old Rita Edwards who achieved an exceptional outcome with IDD Therapy after suffering for four years with an L1/2 disc bulge which surgeons would not operate on. She had undergone countless manual treatments, facet joint injections and epidural injections without any lasting improvement. After a series of IDD treatments she became pain and spasm-free and was able to return to work and carry out her daily household chores again.



