IDD Therapy Spinal Decompression vs Traction This article examines the physics and mechanics of how IDD Therapy Spinal Decompression is able to distract and mobilise specfic segments of the spine and thus decompress a targeted intervertebral disc.
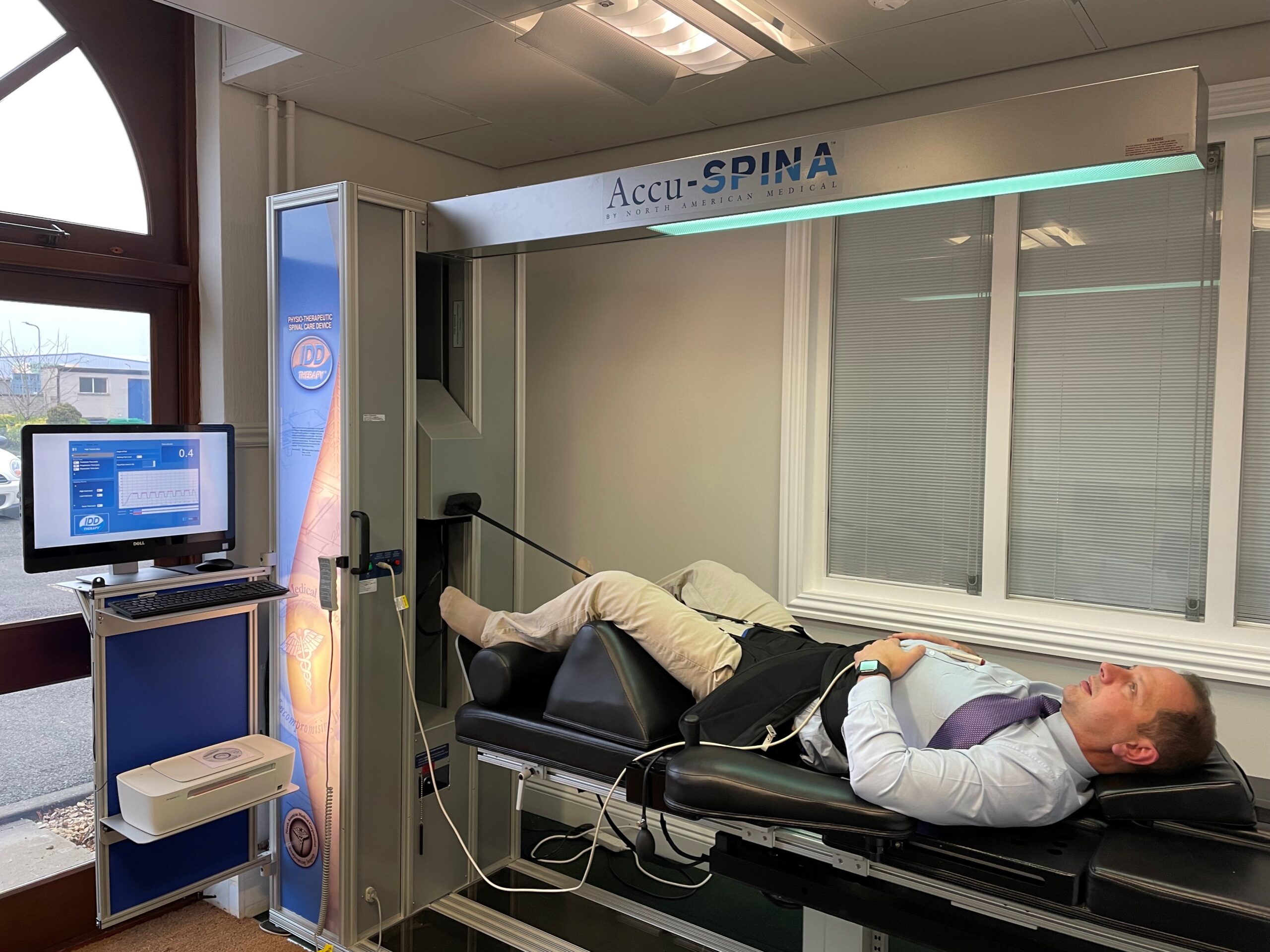
The four goals of IDD Therapy spinal decompression are to: – Release pressure on nerves IDD Therapy treatment is applied by distracting and mobilising targeted spinal segments at precisely measured angles, using high distraction forces which incorporate joint mobilisation in a longitudinal plane. Controlled forces are high enough to comfortably stretch the paraspinal tissues, open and create pressure differentials in the disc space and are applied for sufficient time to have a therapeutic effect. Ergonomic pelvic and thoracic harnesses secure the patient to the bed and a computer controlled cyclic distraction force is applied. Treatment is delivered by CE & FDA cleared Class II SPINA devices. All aspects of treatment and outcomes are recorded as part of a commitment to evidence-based medicine.
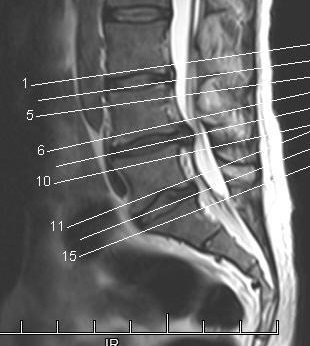
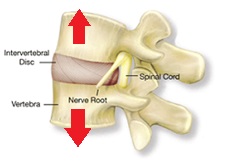
Decompression of a Targeted Spinal Segment. In order to decompress a targeted level, engineers applied the principles of vector forces from physics to the spine. They observed that by focussing a controlled distraction force at a specific angle, they could open targeted spinal segments by between 5mm -7mm (1).
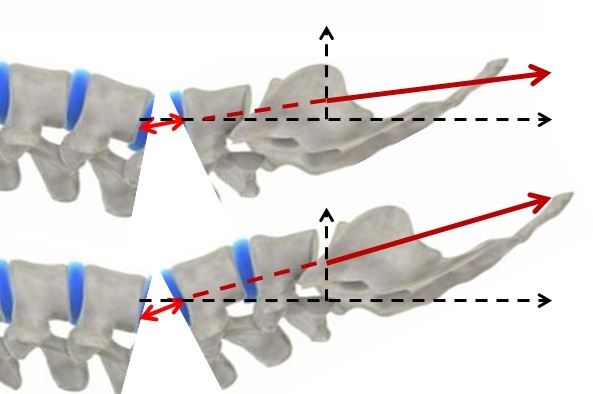
As the angle which a pulling force makes with the horizontal increases, the component of force in the horizontal direction (Fx) decreases and the vertical component of force (Fy) increases.
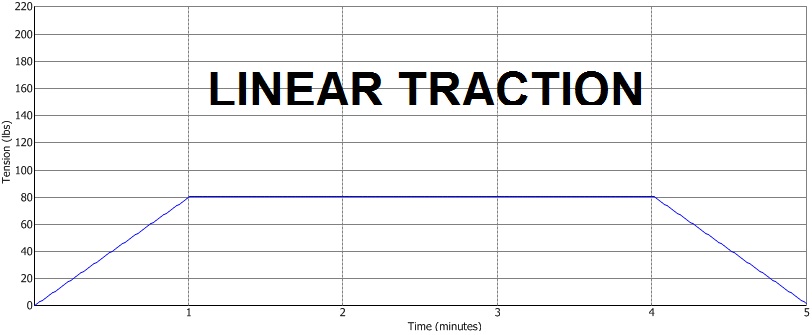
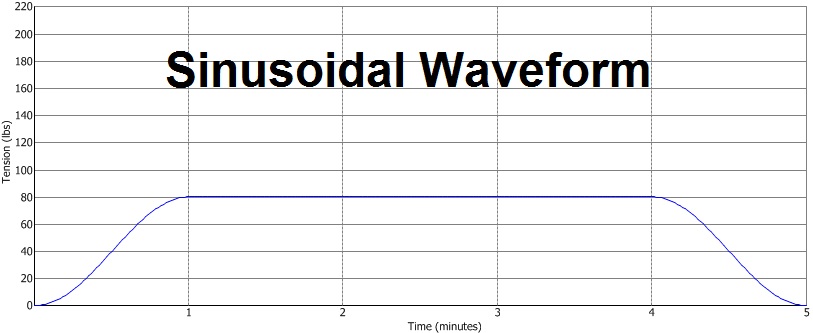
Measured changes in the angle of applied pulling force enable clinicians to focus and direct distraction forces accurately to injured spinal segments. A difference of just 5 degrees can have a bearing on the patient experience. Traditional traction was applied without thought to measuring angles to treat targeted segments. Without this knowledge, practitioners were in effect treating blindly. Sinusoidal distraction force: This patented waveform replaces linear pulling forces allowing greater comfort and application of higher distraction forces of up to half body weight plus 5-10kgs. Patient comfort was a shortcoming for some traction machines and the risk of applying adequate force to distract the spine was that the patient could go into spasm, causing an actual increase in intradiscal pressure and pain.
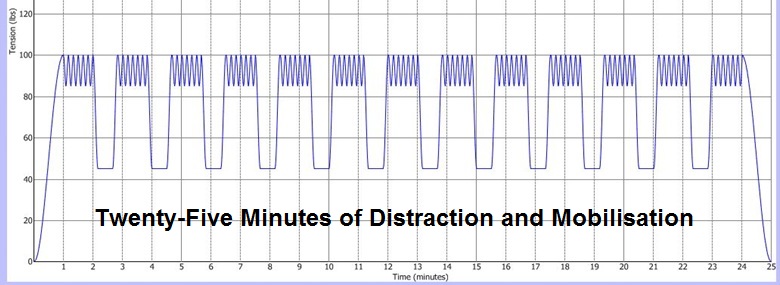
Longer treatment duration: Twenty-five minute treatment during which time joints are distracted for 13 times to a high tension, whilst soft tissues are worked and remain under constant tension. With traditional traction, not only was it uncomfortable for patients to tolerate higher distraction forces for adequate time (necessary to open the disc space), traction was applied for shorter periods to accommodate other treatment techniques within a standard 30 minute treatment slot. Thus whilst some patients might feel some comfort during traction, traction was applied for insufficient time to have an adequate therapeutic effect. A case of fitting the treatment to the needs of the clinic timetable rather than to the therapeutic objectives of treatment which require a longer treatment time.
When mobilising any other joint in the body, clinicians open the joint and then apply mobilisation to so not to rub the joint surfaces and to create a sinovial pumping mechanism. The challenge with the spine is to not only distract the vertebrae longitidinally to decompress the disc, but also to apply adequate force, hold it and then mobilise at the point of maximum distraction.
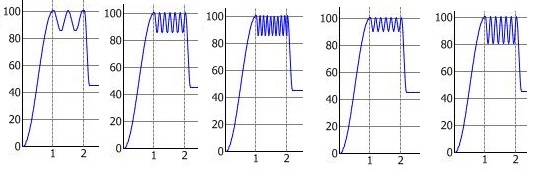
Low frequency Mid Frequency High Frequency Low Amplitude High Amplitude Scanning
Traditional traction was applied in most cases with a try it and see approach without the benefit of a scan. IDD Therapy providers know that a patient with a severely degenerated disc will take longer to notice changes than a patient with a large disc prolapse. With traction, not only did the clinician have an inadequate tool to treat targeted segments, they didn’t have the benefit of seeing the underlying pathology. Thus if a patient did not respond to treatment after a few sessions, that may not have implied that the treatment was ineffective, rather that the treatment plan had not taken account of the condition and likely response time! The sum of the parts: Improved harnessing secures the pelvis, measured angle of distraction, computer controlled sinusoidal waveform, cyclical distraction, higher distraction forces, ergonomic harnesses, patient completely relaxed for 25 minutes, plus benefit of a scan to determine the treatment plan. SUMMARY In order to decompress (take pressure off) a joint, it is necessary to distract it in the opposite direction to the compressive force. Where a joint has become stiff and immobile, gentle mobilisation at the point of distraction helps to improve mobility in the joint and allow the natural mechanisms which keep joints healthy to operate freely. IDD Therapy Spinal Decompression applies new technology to physical laws to enable clinicians to distract and mobilise targeted spinal segments as part of a complete programme of care, including manual therapy and exercise rehabilitation. 1 Shealy N, Leroy P: New Concepts in Back Pain Management. AJPM (1) 20:239241 1998 |